Defining and Defending a Blood Pressure in the Operating Room & Intensive Care Unit
Despite surgical patients presenting to the operating room (OR) sicker than ever before, the intraoperative period has, paradoxically, become far safer. Current estimates of intraoperative mortality are less than 1 in 100,000 patients (1). However, 30-day postoperative mortality is still significant at 1-2%, a fact that suggests that if 30-day postop mortality were considered a disease, it would be the third leading cause of death in the United States (2).
There are few interventions that anesthesiologists and intensivists can offer that have direct evidence of improved patient survival. The one goal of anesthetic management over the years has been hemodynamic stability. There is now, more than ever before, direct evidence of the damaging effects of low blood pressure. These effects are clearly associated with myocardial injury, mortality and acute kidney injury. In addition, these effects extend beyond the operating room, into the post-surgical recovery wards and for the critically ill patient in the intensive care unit (ICU). Appropriate definition of threshold pressures in the operating room and ICU and a rationale strategy for defending these is of utmost importance in current practice.
Intraoperative Blood Pressure
Even brief periods of mild intraoperative hypotension (at thresholds that were previously considered tolerable) are harmful. Once mean arterial pressure (MAP) reaches 55 mmHg, only a few minutes of exposure is associated with myocardial and renal injury.(3) Minimum intraoperative MAP maintained for ten minutes at less than about 70 mmHg is strongly associated with mortality (Fig. 1).(4) There are similarly strong associations between hypotension and myocardial injury (MAP threshold 65 mmHg) (Fig. 2A) and kidney injury (MAP threshold 75 mmHg).(5) Importantly, these relationships are maintained when MAP is expressed as a percentage of baseline blood pressures. (Fig. 2C) In an analysis of adults having non-cardiac surgery at the Cleveland Clinic, a full third of all hypotension, (MAP threshold <65 mmHg), occurred in the post-induction to pre-surgical incision period. The hypotensive insult was significantly and comparably associated with both myocardial and kidney injury before and after incision (6). Knowing that this hypotension before incision results almost exclusively from anesthetic drugs, suggests that it should be largely preventable. A major limitation of these large datasets is their observational nature. Unfortunately, this means that there exist both known and unknown confounding factors and which are related to both exposure and outcome. Therefore, the reported hypotension may simply be a marker of underlying illness rather than a mediator of harm.
Randomized trials of intra-operative blood pressure control are rare and difficult to conduct. Notably, recent work by the INPRESS investigators lead by Futier and colleagues compared tight vs. minimal intraoperative blood pressure control (n=298).(7) High-risk patients were randomized to minimal blood pressure control (ephedrine for systolic pressure <80 mmHg or <40% below baseline) vs. a norepinephrine infusion to maintain systolic pressure within 10% of baseline values during and for four hours after surgery. The primary outcome, a composite of systemic inflammatory response syndrome and/or at least one organ failure, occurred in 56/147 patients in the norepinephrine (tight control) group vs 75/145 patients in the minimal control group: relative risk 0.73 (95% CI: 0.56, 0.94). The intervention threshold of a systolic pressure of 80 mmHg is low compared to what most anesthesiologists would react to in real life. It is very likely that a higher intervention pressure presumably would have reduced the observed 25% benefit. Blood Pressure in the Critically Ill Patient in Intensive Care Units Hypotension in critical care units may be profound, prolonged and especially damaging because of several co-existing, complicated and often cumulative other insults. Similar to the intraoperative period, there is increasing evidence for an association between hypotension at thresholds that seem to challenge the general norm of 65 mmHg established by the surviving sepsis campaign guidelines and serious complications. (8-10)
At the Cleveland Clinic, we recently evaluated a cohort of 2,918 postoperative critical care patients and saw an association between the lowest recorded MAP and a primary composite of myocardial injury and in-hospital mortality at 7 days. At MAP less than 90 mmHg, every 10-mmHg difference between patients in the lowest MAP on any given day increased the risk of the primary composite by about 50%.(8) (Fig.3) Hypotension and acute kidney injury was linearly related over the entire range of MAP from 50 mmHg to 110 mmHg, with an adjusted overall hazard ratio of 1.16 (1.29 for stage 2&3 acute kidney injury) per 10-mmHg reduction in the lowest recorded MAP.
We have also shown that both the duration and severity of hypotension matter. For example, an hour of exposure to 80 mmHg was similar in damage to even a few minutes below 70 mmHg.(8) Whereas these data were from a postoperative (mostly non-septic) patient cohort, another recent examination of nearly 9,000 septic patients across 110 ICUs in the United States saw a similar signal for harm at a higher threshold MAP. Specifically, this study saw that the risks for mortality, AKI, and myocardial injury first developed at a MAP of 85 mmHg, and the risk of mortality and AKI progressively worsened at lower blood pressures, on a MAP range from 55-85 mmHg.(Fig. 4)(9) Other smaller cohorts have also reported MAP-associated organ system injury at thresholds normally considered safe in the surgical and mixed ICU populations. (11) (12) (13) (14) It is worth keeping in mind, however, that the interpretation of all these hypotension data is complicated by sepsis. Because sepsis results in both hypotension and organ system injury from independent, although related, mechanisms, significant dependent-variable confounding occurs in all of these analyses.(15)
Interestingly, hypotension in critical care units has also been associated with delirium. Aldemir and colleagues screened 818 critical care patients daily for 10 days and reported an association between systolic pressure <80 mmHg and delirium.(16) Likewise, at the Cleveland Clinic, we have seen that a 10-mmHg reduction in the lowest MAP on each day during ICU stay at a MAP of less than 65 mmHg was significantly associated with a higher hazard of delirium, with an adjusted hazard ratio 1.16 (95% CI: 1.07, 1.26; P<0.001) (unpublished data-Cleveland Clinic). Only one large multicenter randomized controlled trial of different blood pressure targets has been performed to date. In that study, no difference in mortality was note for blood pressure targets of 80-85 mmHg or 65-70 mmHg in patients with septic shock.(17) However, a closer look at this work shows that the actual blood pressure targets achieved were different (85-90 mmHg vs. 70-75 mmHg) from experimental design, making it difficult to answer questions about hypotension from this published work. In addition, there were no assessment of myocardial injury (MINS) based on systematic collection of troponin bioanalysis and clinical myocardial infarction were only observed in 9 patients which precluded reliable assessment of this important outcome. Other important findings from this landmark work were that atrial fibrillation was more common in patients assigned to higher blood pressure and patients with chronic hypertension who were assigned to the lower pressure target had more renal injury and the prevalence of renal replacement therapy was higher in this subgroup. This study and other smaller studies have significantly associated higher blood pressure targets with more cardiac arrhythmias and vasopressor use, without detecting a difference in serum lactate, regional blood flow, or mortality compared with lower blood pressure targets.(18-21)
Conclusions
Today, the available data suggests that MAP well above the established norm of 65 mmHg (and possibly higher than the threshold for the operating room) are needed to prevent hypotensive organ injury in postoperative critical care patients, including those who are septic.(8, 9, 22) A plausible explanation relates to the need for increased perfusion pressures in critically ill patients who have coexisting acute insults in the setting of complex chronic conditions, including extreme sympathetic stimulation, fluid shifts, nutritional deficits, infectious diseases and hypermetabolic/hypercatabolic states. While previous concern for arrhythmias when pushing higher MAP targets using catecholamine mono-therapy may have been appropriate, it may be possible to achieve higher MAPS without this risk due to the recent advent, approval and adoption of newer, more potent (non-catecholamine) vasopressors such as Angiotensin II.(23)
Overall, we may be correct in defining a harm threshold of MAP of about 65 mmHg in the intraoperative period, and possibly considerably greater in critical care units; however, it also seems likely that this may not be an adequate threshold in all patient groups. The available data is largely retrospective and has several concerns for confounding. While this concise review covers the most recent work in this area, readers are also referred to a comprehensive overview of all contemporary published literature & relevant trials.(22) Randomized data is sparse, but suggests that at least some harm can be prevented by intervening to limit the severity and duration of even mild hypotension. The message remains loud & clear for Critical Care Anesthesiologists: “Define a MAP and then defend that MAP” whatever clinical setting your patient may be in.
References
- Lienhart A, Auroy Y, Pequignot F, Benhamou D, Warszawski J, Bovet M, Jougla E: Survey of anesthesia-related mortality in France. Anesthesiology 2006, 105(6):1087-1097.
- Bartels K, Karhausen J, Clambey ET, Grenz A, Eltzschig HK: Perioperative organ injury. Anesthesiology 2013, 119(6):1474-1489.
- Walsh M, Devereaux PJ, Garg AX, Kurz A, Turan A, Rodseth RN, Cywinski J, Thabane L, Sessler DI: Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: Toward an empirical definition of hypotension. Anesthesiology 2013, 119(3):507-515.
- Mascha EJ, Yang D, Weiss S, Sessler DI: Intraoperative mean arterial pressure variability and 30-day mortality in patients having noncardiac surgery. Anesthesiology 2015, 123:79-91.
- Salmasi V, Maheshwari K, Yang D, Mascha EJ, Singh A, Sessler DI, Kurz A: Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: A retrospective cohort analysis. Anesthesiology 2017, 126(1):47-65.
- Maheshwari K, Turan A, Mao G, Yang D, Niazi AK, Agarwal D, Sessler DI, Kurz A: The association of hypotension during non-cardiac surgery, before and after skin incision, with postoperative acute kidney injury: a retrospective cohort analysis. Anaesthesia 2018.
- Futier E, Lefrant JY, Guinot PG, Godet T, Lorne E, Cuvillon P, Bertran S, Leone M, Pastene B, Piriou V et al: Effect of individualized vs standard blood pressure management strategies on postoperative organ dysfunction among high-risk patients undergoing major surgery: A randomized clinical trial. Jama 2017, 318(14):1346-1357.
- Khanna A, Mao G, Liu L, Yang D, Perez-Protto S, Chodavarapu P, Schacham Y, Mascha E, Sessler D: 177: HYPOTENSION INCREASES ACUTE KIDNEY INJURY, MYOCARDIAL INJURY AND MORTALITY IN SURGICAL CRITICAL CARE. Critical Care Medicine 2018, 46(1):71.
- Maheshwari K, Nathanson BH, Munson SH, Khangulov V, Stevens M, Badani H, Khanna AK, Sessler DI: The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Intensive care medicine 2018.
- Asfar P, Radermacher P, Ostermann M: MAP of 65: target of the past? Intensive care medicine 2018.
- Badin J, Boulain T, Ehrmann S, Skarzynski M, Bretagnol A, Buret J, Benzekri-Lefevre D, Mercier E, Runge I, Garot D et al: Relation between mean arterial pressure and renal function in the early phase of shock: a prospective, explorative cohort study. Critical care (London, England) 2011, 15(3):R135.
- Poukkanen M, Wilkman E, Vaara ST, Pettila V, Kaukonen KM, Korhonen AM, Uusaro A, Hovilehto S, Inkinen O, Laru-Sompa R et al: Hemodynamic variables and progression of acute kidney injury in critically ill patients with severe sepsis: data from the prospective observational FINNAKI study. Critical care (London, England) 2013, 17(6):R295.
- Dunser MW, Takala J, Ulmer H, Mayr VD, Luckner G, Jochberger S, Daudel F, Lepper P, Hasibeder WR, Jakob SM: Arterial blood pressure during early sepsis and outcome. Intensive care medicine 2009, 35(7):1225-1233.
- Varpula M, Tallgren M, Saukkonen K, Voipio-Pulkki LM, Pettila V: Hemodynamic variables related to outcome in septic shock. Intensive care medicine 2005, 31(8):1066-1071.
- Bagshaw SM, George C, Bellomo R: Early acute kidney injury and sepsis: a multicentre evaluation. Critical care (London, England) 2008, 12(2):R47.
- Aldemir M, Ozen S, Kara IH, Sir A, Bac B: Predisposing factors for delirium in the surgical intensive care unit. Critical care (London, England) 2001, 5(5):265-270.
- Asfar P, Meziani F, Hamel JF, Grelon F, Megarbane B, Anguel N, Mira JP, Dequin PF, Gergaud S, Weiss N et al: High versus low blood-pressure target in patients with septic shock. N Engl J Med 2014, 370(17):1583-1593.
- Bourgoin A, Leone M, Delmas A, Garnier F, Albanese J, Martin C: Increasing mean arterial pressure in patients with septic shock: effects on oxygen variables and renal function. Crit Care Med 2005, 33(4):780-786.
- Thooft A, Favory R, Salgado DR, Taccone FS, Donadello K, De Backer D, Creteur J, Vincent JL: Effects of changes in arterial pressure on organ perfusion during septic shock. Critical care (London, England) 2011, 15(5):R222.
- Lamontagne F, Meade MO, Hebert PC, Asfar P, Lauzier F, Seely AJE, Day AG, Mehta S, Muscedere J, Bagshaw SM et al: Higher versus lower blood pressure targets for vasopressor therapy in shock: a multicentre pilot randomized controlled trial. Intensive care medicine 2016, 42(4):542-550.
- LeDoux D, Astiz ME, Carpati CM, Rackow EC: Effects of perfusion pressure on tissue perfusion in septic shock. Crit Care Med 2000, 28(8):2729-2732.
- Sessler DI, Khanna AK: Perioperative myocardial injury and the contribution of hypotension. Intensive care medicine 2018, 44(6):811-822.
- Khanna A, English SW, Wang XS, Ham K, Tumlin J, Szerlip H, Busse LW, Altaweel L, Albertson TE, Mackey C et al: Angiotensin II for the Treatment of Vasodilatory Shock. N Engl J Med 2017, 377(5):419-430.
Figures
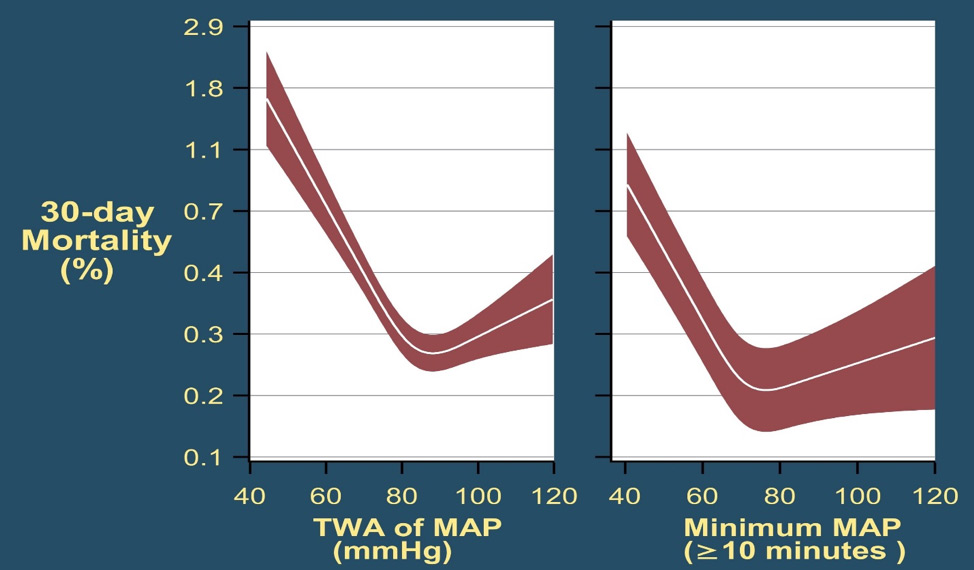
Fig. 1: Mortality in the 30 post-operative days as a function of time-weighted average (TWA) mean arterial pressure or lowest mean pressure maintained for at least 10 minutes. With permission from Mascha et al: Intraoperative mean arterial pressure variability and 30-day mortality in patients having noncardiac surgery. Anesthesiology 2015; 123: 79-91

Fig. 2: The left graph (A) shows the relationship between the lowest cumulative absolute mean arterial pressure maintained for 1, 3, 5, and 10 minutes and myocardial injury. The right graph (C) shows the relationship between the lowest cumulative relative mean arterial pressure maintained for 1, 3, 5, and 10 minutes and myocardial injury. Both were highly predictive, but relative thresholds were not more predictive than absolute thresholds which are easier to use. The relationships were generally similar for acute kidney injury (not shown). With permission from Salmasi, et al: Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: A retrospective cohort analysis. Anesthesiology 2017; 126: 47-65.
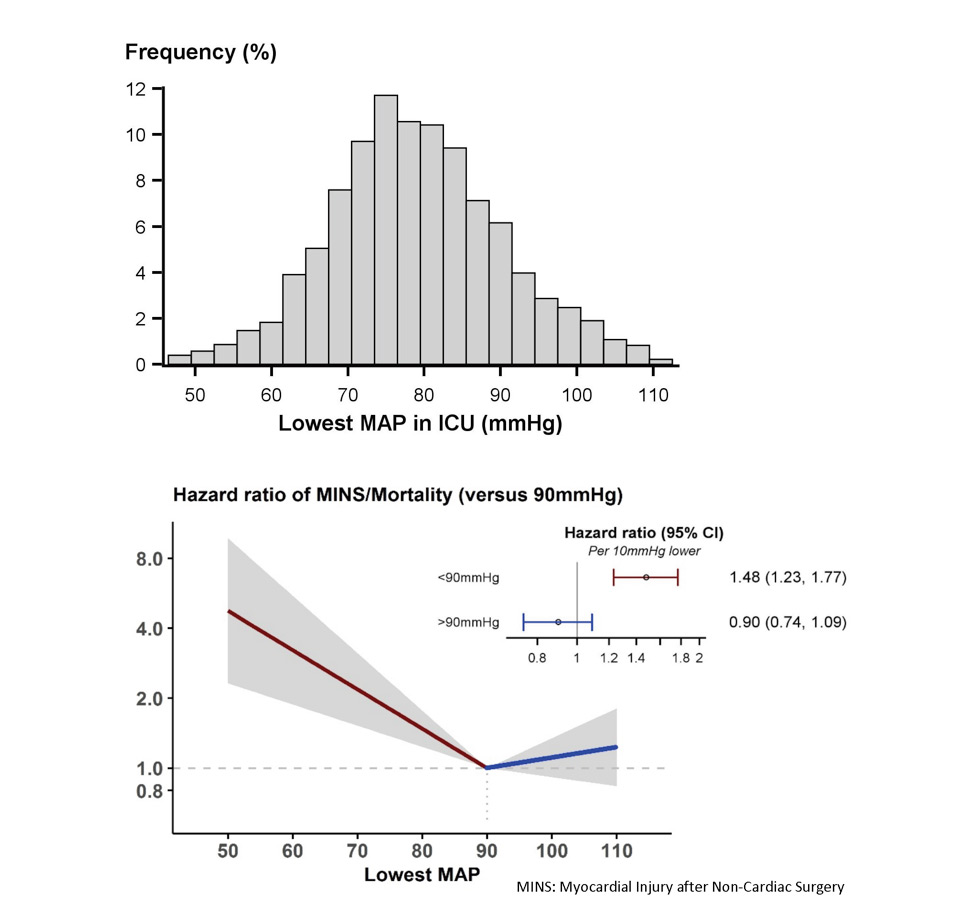
Fig. 3: Association of exposure to hypotension at mean arterial pressures (MAP) less than 90 mm Hg and a primary composite outcome of myocardial injury after non-cardiac surgery (MINS) and mortality. For any two postoperative patients in the surgical ICU with a 10 mm Hg difference in the lowest MAP per day of less than 90 mmHg there was a nearly 50% increase in the hazards of the primary outcome. With permission from Khanna AK et al: Hypotension increases acute kidney injury, myocardial injury and mortality in surgical critical care. Critical Care Medicine 2018, 46(1):71. (Presented at SCCM 2018, San Antonio, TX)
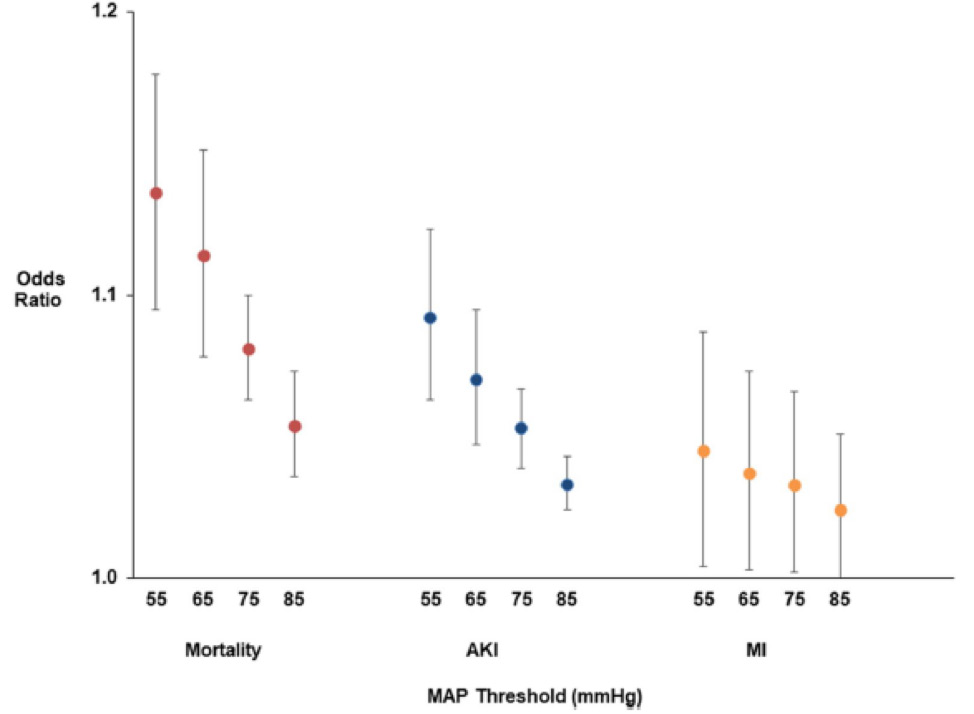
Fig. 4: Association of hypotension exposure with in-hospital mortality, AKI and myocardial injury. Adjusted odds ratios and 95% confidence intervals for a 1 mmHg increase in TWA-MAP, below different thresholds are shown for the primary outcome of in-hospital mortality and secondary outcomes of acute kidney injury and myocardial injury. With permission from Maheshwari, et al: The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Intensive Care Med. 2018 Jun 5. doi: 10.1007/s00134-018-5218-5. [Epub ahead of print]
Author

Categories
- Announcements
- Annual Meeting
- Award
- Book & Media Reviews
- Call for Articles
- Case Reports
- Clinical Research Consortium
- Committee Reports
- Council Report
- COVID-19
- DEI
- Early Career Intensivists
- Editor’s Message
- Featured Articles
- Fellows
- Jobs
- Literature Survey
- Match Applicants
- Medical Ethics
- Member Essays
- Member Spotlight
- Opinion
- Patient Safety Series
- PDAC
- President’s Corner
- Private Practice
- Pro/Con
- Research Updates
- Social Media Highlights
- Submission Guidelines
- Topical Review
- Wellness Series
- White Papers
- Women in Critical Care
- Work-Life Balance
Current Newsletter

Past Newsletters
Drip
















ASA 2023 Annual Meeting







September is Women in Medicine Month and throughout the month, four of our members will be sharing their experiences as a woman in critical care.




IARS & SOCCA Abstracts 2023
Abstracts of International Anesthesia Research Society & Society of Critical Care Anesthesiologists 2023 Annual Meetings are available in the May 2023 issue of Anesthesia & Analgesia.

Podcasts
SOCCA Women in Critical Care has collaborated with Stanford Continuing Medical Education for a Stanford Medcast Women in Critical Care podcast mini-series.
Episode #66—”Psychosocial Challenges Facing Physicians”—stream now
SOCCA polled the WICC and got the answers we wanted to hear about. We hope this episode helps at least one person out there!
If you have 21 minutes, listen and get your CME credit!

Episode #65—”Stereotype Threats”—stream now

Episode #63: “The Wicked Problem of Physician Well-Being”—stream now

Episode #59—“Underestimation of Influence”—stream now



