Clinical Considerations for Airway Management in Patients with Ankylosing Spondylitisby Anoop Chhina, MD, William Peruzzi, MD, and John Reveille, MD
Volume 33 | Issue 4 NewsletterAnkylosing Spondylitis (AS) is an inflammatory rheumatic disease that primarily affects the spine, although other joints and organs can become involved. AS and its parent disease, Axial Spondyloarthritis, are not rare, and affect at least 2 million and 5.9 million adults in the United States alone, respectively (1,2,3). Anatomic and Physiologic Airway Changes Resulting from Ankylosing Spondylitis Patients with AS may have ossification of the spinal ligaments and calcification of the outer fibers of the annulus fibrosis of the intervertebral disc, which leads to a “bamboo” appearance of the spine on radiographic images (Figure 1). Fusion of the apophyseal joints and extensive syndesmophyte formation usually leads to fixed forward kyphosis and loss of mobility of the thoracic and cervical spine.(4,21) Cervical involvement occurs in more than 50% of patients with AS (5), and by 20 years of disease progression, more than 70% of patients have cervical involvement. (Figure 1) Intubation is challenging for patients with AS because they may have (1) limited atlanto-occipital extension, (2) limited mouth opening, and (3) an inability to lie supine secondary to both fusion and anterior flexion of the cervical spine. Osteoporosis is common in patients with AS, present in up to 61%, and is associated with increased risk for spinal fracture, especially in those with long disease duration and advanced spinal disease (6,19). Also, recent data have shown that patients with AS have an increased risk of developing a vertebral fracture even after adjusting for age, gender, and the presence of osteoporosis (7). All of these physiological changes incurred by AS can combine and lead to a spinal structure with mechanics that mimic a long lever arm that is susceptible to low energy trauma (4), including the forces generated by direct laryngeal visualization during intubation. A fused, anteriorly positioned and flexed cervical spine combined with ossified supporting ligaments may not safely tolerate a chin lift, jaw thrust, or direct laryngoscopy required to pass an endotracheal tube. Case reports have highlighted an occurrence of severe neurological deficits, including permanent tetraplegia secondary to direct laryngoscopy in this patient population (8). AS involvement of the temporomandibular joint results in a narrowing of the joint space due to the presence of osteophytes and erosion of joint (9), which can severely impede mouth opening and impede any type of transoral approach to the larynx. Historically, it is believed that Pharaoh Ramses II (1303-1213 BCE) had AS. His neck had to be hyperextended to fit into his sarcophagus (Figure 2), which resulted in cervical spinal fracture (Figure 3) (10). Airway Management Considerations for Patients with Ankylosing Spondylitis Airway management in the hospital setting for patients with AS requires an individualized approach, always consider the patient’s overall clinical condition, their specific airway anatomy, available equipment, and caregiver skills. Patients with chronic cervical kyphosis from AS have a significant risk of neurological injury from any neck-extending procedure. Neck extension can also cause vertebrobasilar insufficiency resulting from bony encroachment on the vertebral artery. Injuries to the cervical spine and spinal cord after an emergency intubation in patients with AS, such as dislocation of C6 vertebra and tetraparesis, have been reported (12). Direct laryngoscopy is associated with a low first pass success rate and a high complication rate in patients with AS; hence, this technique should be avoided whenever possible. However, video-laryngoscopes provide an easy learning curve with reasonable effectiveness and safety comparable to standard fiberoptic intubation in some situations (11). If the patient has a significant level of temporomandibular joint damage with limited oral opening, or significant fixed cervical spine deformities are present, the video-laryngoscope may not be any safer or effective than direct laryngoscopy. In these situations, fiberoptic intubation will be the best approach. In emergent situations, intubating LMA (I-LMA) will be helpful (14,15,20). The advantages of this technique are that laryngeal visualization is not necessary, the trachea can be intubated without head or neck movement, and ventilation of the patient’s lungs can be maintained during the procedure. Other Considerations Regarding Care of Patients with Ankylosing Spondylitis Pulmonary Considerations: Patients with AS may have restrictive lung disease due to fusion of costovertebral joints, which can limit chest expansion. Additionally, patients with AS may have pulmonary fibrosis, which often manifests the worst in the upper lobes. Therefore, pulmonary function tests and arterial blood gas analysis for patients with AS are advisable, especially during preoperative preparations. Cardiac Considerations: In patients with AS, inflammatory involvement of the heart just under aortic valve can lead to aortic valvular insufficiency, or even complete heart block; thus, a preoperative electrocardiogram is mandatory, and an echocardiogram should be obtained to assess the severity of possible AS–associated valvular disease. Complications Associated with Spinal Cord Injury in Patients with Ankylosing Spondylitis In an analysis of 12,484 hospital admissions and 267 deaths in patients with AS, data abstracted from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample between 2007 and 2011 showed that c-spine fracture with spinal cord injury and sepsis led to the highest odds of death (16). Another recent analysis of the U.S. Nationwide Inpatient Sample data of years 2016-2018 of 5385 AS patients with spinal fractures found spinal cord injury was present in 26.5% of the patients with cervical spine fractures. The overall complication rate was 40.8%, highest in those with spinal cord injury. Respiratory complications, including pneumonia and respiratory insufficiency, were the predominant complications in the overall cohort. Prone Positioning in Patients with Ankylosing Spondylitis Without proper planning, these patients may experience disastrous outcomes, such as complete spinal cord damage and possible death. Prone positioning can lead to physiological damage to patients with AS if underlying restrictive lung disease or cervical spine fracture are present (16,17). Therefore, proper planning and discussion needs to take place between care teams if prone positioning is absolutely necessary. Ideally, special positioning beds with proper padding and head support should be used to maintain the curvature of spine, and any forcible movements of the neck in the presence of neuromuscular blockade should be avoided (18). References
 Figure 1. Lateral Cervical Spine Radiograph of a Patient with Advanced AS. Note the Fusion of the Apophyseal Joints Posteriorly and of the Outer Fibers of the Annulus Fibrosus Anteriorly
 Figure 2. The Remains of Pharaoh Ramses II, Indicating the Pre-Mortem Position of the Neck and the Forced Hyperextension of the Cervical Spine to Fit into the Sarcophagus
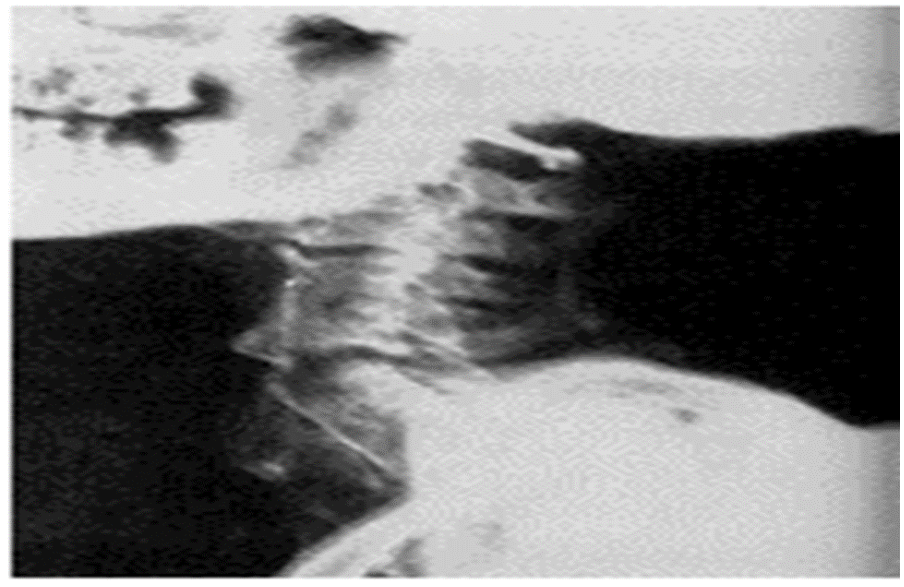 Figure 3. Lateral Spinal Radiograph of Ramses II: The Results of Forced Hyperextension of a Fused Cervical Spine Authors |


