Case Report: Successful Management of Right Ventricle Perforation Associated with a Protek Duo Cannula Placement
Introduction:
Acute right ventricular failure (RVF) due to post-left ventricular assist device (LVAD) placement is challenging to treat with the management often limited to placement of either surgical or percutaneous mechanical circulatory devices. The Protek Duo® (LivaNova) is a percutaneous right ventricular support device (RVAD), which due to its relative ease of placement, has been a breakthrough in the management of post-LVAD implantation acute RVF. 1
Cardiac perforation from placement of a Protek Duo cannula is a rare but potentially lethal complication. This case is the first to describe a patient who developed cardiac tamponade from a Protek Duo cannula perforation of the right ventricle. The report discusses preoperative and intraoperative management of this condition and relevant transesophageal echocardiography (TEE) imaging that aided in the diagnosis and surgical repair of the perforation.
Case Summary:
A 76 year-old male with a history of heart failure with reduced ejection fraction secondary to ischemic cardiomyopathy was admitted for an elective surgical Heartmate III LVAD and Protek Duo cannula placement. A preoperative transthoracic echocardiogram (TTE) completed on hospital admission revealed an ejection fraction of 10% with a known left ventricular thrombus and preserved right ventricular function. The patient proceeded to the operating room (OR), and he underwent successful implantation of a HeartMate III, closure of a patent foramen ovale, and placement of a 29-French Protek Duo cannula. Intraoperative TEE revealed normal right ventricular function and a Protek Duo cannula positioned with the tip in the right pulmonary artery without any outflow obstruction. The chest remained open, and he was transferred to the cardiovascular intensive care unit (CVICU) in a hemodynamic stable condition.
On post-operative day (POD) 4, the patient went to the OR for a scheduled chest closure, and he returned to the CVICU in stable condition. Several hours later, the patient became acutely hypotensive, with an accompanying decrease in Protek Duo flows, increase in central venous pressure (CVP), and increase in chest tube output. The patient was emergently taken to the OR for chest exploration, with concerns for possible cardiac tamponade.
Utilizing both direct visualization (Figure 1) and intraoperative TEE imaging, a right ventricular perforation was identified, as the Protek Duo cannula had eroded through the right ventricle creating a linear perforation along the ventricular free wall. After successful surgical repair of the ventricular perforation, there was a subsequent decrease in Protek Duo flows to 0.5 L/min, an increase in the CVP to 20 mmHg, and right atrial distention was noted on TEE (Figure 2). After interrogation of both the Protek Duo inflow and outflow circuits and the oxygenator, the decision was made to replace the Protek Duo device.
After successful wean of the Protek Duo device, the patient returned to the OR on POD 10 for RVAD removal. The patient had an overall complex hospital course, and was discharged to inpatient rehabilitation on POD 128.
Case Discussion:
Ventricular perforation due to a mechanical device implantation is an uncommon but potentially life-threatening complication of cardiac surgery. Very few cases of ventricular perforation have been reported in the literature. Most cases of cardiac perforation are related to the placement of cardiac implantable electronic devices (CIEDs), with the incidence of cardiac perforation ranging from 0.1% to 0.8% for pacemakers and 0.6% to 5.2% for implantable cardiac defibrillators. 2 Cardiac perforation is classified as acute when it occurs within 24 hours of device implantation, subacute perforation occurring between 1 day and 30 days, or chronic perforation occurring more than 30 days after implantation. Subacute ventricular perforation is rare, and affects 0.5% to 1.2% of patients with CIEDs. 3 In these cases, perforation most often occurs in the right ventricle apex or free wall of the right ventricular outflow track, where the wall is thinner than other structures of the heart. 4
Although perforation has been reported with CIEDs, very little is known about the risk of myocardial perforation in patients with percutaneous mechanical circulatory devices. This is the first case to our knowledge regarding right ventricular free wall perforation in a patient with a recent Protek Duo cannula placement. In our case, the perforation occurred in the subacute setting on POD 4 after a successful and uneventful insertion several days prior. The patient showed signs of hemodynamic instability yet was taken to the OR promptly before he could clinically worsen. The clinical presentation of ventricular perforation varies from cardiac tamponade and hemodynamic instability to incidental discovery on imaging, where prompt recognition of this condition and emergent surgical intervention are crucial for patient survival. 2,3
References:
- Bhatia M, Jia S, Smeltz A, Kumar PA. Right Heart Failure Management: Focus on Mechanical Support Options. J Cardiothorac Vasc Anesth. 2022;36(8 Pt B):3278-3288. doi:10.1053/j.jvca.2022.02.022
- Elbatran AI, Akhtar Z, Bajpai A, et al. Percutaneous management of lead-related cardiac perforation with limited use of computed tomography and cardiac surgery. Pacing Clin Electrophysiol. 2021;44(4):614-624. doi:10.1111/pace.14204
- Allouche E, Chargui S, Fathi M, Bezdah L. Subacute right ventricle perforation: a pacemaker lead complication. BMJ Case Rep. 2021;14(5):e242489. Published 2021 May 12. doi:10.1136/bcr-2021-242489
- Tarbiat M, Bakhshaei MH, Moradi M. Successful Management of Right Ventricular Perforation Associated with a Pacemaker Lead During Off-Pump CABG Surgery: A Case Report. Anesth Pain Med. 2017;7(4):e57799. Published 2017 Jul 24. doi:10.5812/aapm.57799
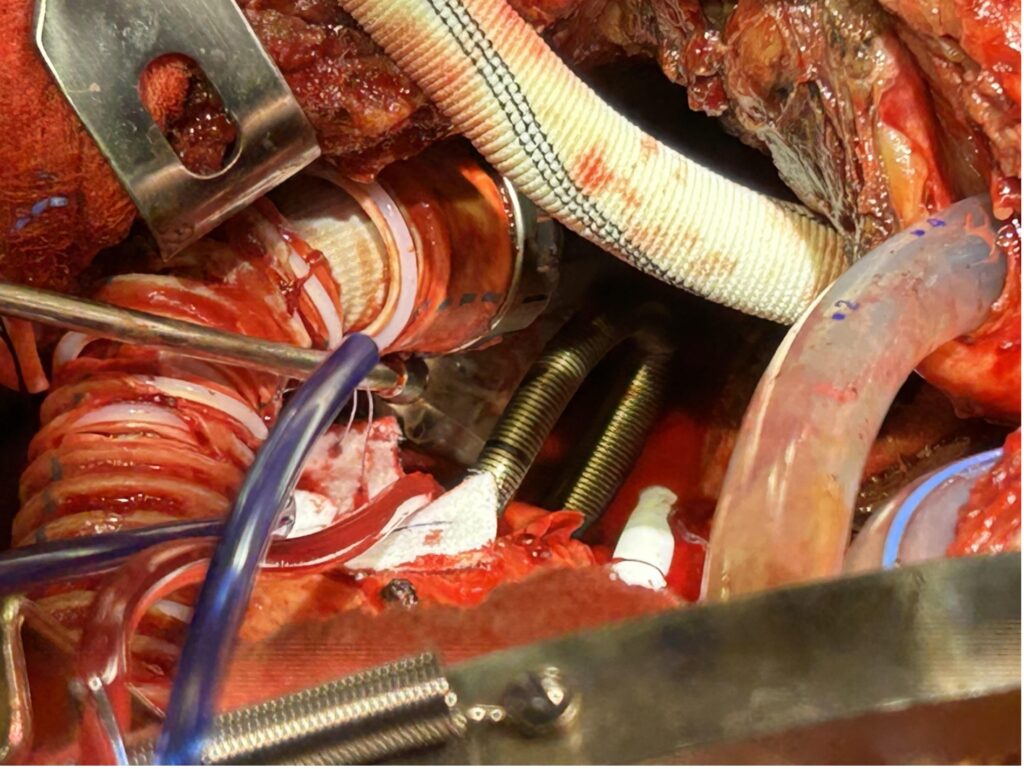
Figure 1: Right ventricular perforation as found intraoperatively on POD 4 where the Protek Duo cannula had eroded through the right ventricle creating a linear perforation along the ventricular free wall
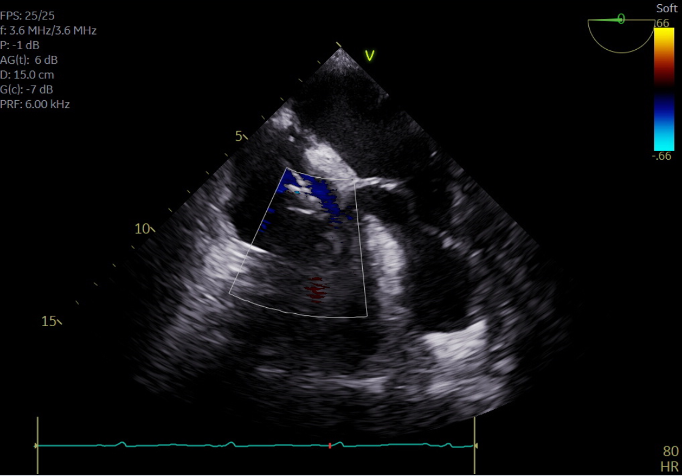
Figure 2: Intraoperative TEE showing Protek Duo cannula placement as well as right atrial distention that was noted after repair of the right ventricular perforation
Authors



Categories
- Announcements
- Annual Meeting
- Award
- Book & Media Reviews
- Call for Articles
- Case Reports
- Clinical Research Consortium
- Committee Reports
- Council Report
- COVID-19
- DEI
- Early Career Intensivists
- Editor’s Message
- Featured Articles
- Fellows
- Jobs
- Literature Survey
- Match Applicants
- Medical Ethics
- Member Essays
- Member Spotlight
- Opinion
- Patient Safety Series
- PDAC
- President’s Corner
- Private Practice
- Pro/Con
- Research Updates
- Social Media Highlights
- Submission Guidelines
- Topical Review
- Wellness Series
- White Papers
- Women in Critical Care
- Work-Life Balance
Current Newsletter

Past Newsletters
Drip
















ASA 2023 Annual Meeting







September is Women in Medicine Month and throughout the month, four of our members will be sharing their experiences as a woman in critical care.




IARS & SOCCA Abstracts 2023
Abstracts of International Anesthesia Research Society & Society of Critical Care Anesthesiologists 2023 Annual Meetings are available in the May 2023 issue of Anesthesia & Analgesia.

Podcasts
SOCCA Women in Critical Care has collaborated with Stanford Continuing Medical Education for a Stanford Medcast Women in Critical Care podcast mini-series.
Episode #66—”Psychosocial Challenges Facing Physicians”—stream now
SOCCA polled the WICC and got the answers we wanted to hear about. We hope this episode helps at least one person out there!
If you have 21 minutes, listen and get your CME credit!

Episode #65—”Stereotype Threats”—stream now

Episode #63: “The Wicked Problem of Physician Well-Being”—stream now

Episode #59—“Underestimation of Influence”—stream now



