Clinical Considerations for Airway Management in Patients with Ankylosing Spondylitis
Ankylosing Spondylitis (AS) is an inflammatory rheumatic disease that primarily affects the spine, although other joints and organs can become involved. AS and its parent disease, Axial Spondyloarthritis, are not rare, and affect at least 2 million and 5.9 million adults in the United States alone, respectively (1,2,3).
Anatomic and Physiologic Airway Changes Resulting from Ankylosing Spondylitis
Patients with AS may have ossification of the spinal ligaments and calcification of the outer fibers of the annulus fibrosis of the intervertebral disc, which leads to a “bamboo” appearance of the spine on radiographic images (Figure 1). Fusion of the apophyseal joints and extensive syndesmophyte formation usually leads to fixed forward kyphosis and loss of mobility of the thoracic and cervical spine.(4,21) Cervical involvement occurs in more than 50% of patients with AS (5), and by 20 years of disease progression, more than 70% of patients have cervical involvement. (Figure 1)
Intubation is challenging for patients with AS because they may have (1) limited atlanto-occipital extension, (2) limited mouth opening, and (3) an inability to lie supine secondary to both fusion and anterior flexion of the cervical spine.
Osteoporosis is common in patients with AS, present in up to 61%, and is associated with increased risk for spinal fracture, especially in those with long disease duration and advanced spinal disease (6,19). Also, recent data have shown that patients with AS have an increased risk of developing a vertebral fracture even after adjusting for age, gender, and the presence of osteoporosis (7).
All of these physiological changes incurred by AS can combine and lead to a spinal structure with mechanics that mimic a long lever arm that is susceptible to low energy trauma (4), including the forces generated by direct laryngeal visualization during intubation. A fused, anteriorly positioned and flexed cervical spine combined with ossified supporting ligaments may not safely tolerate a chin lift, jaw thrust, or direct laryngoscopy required to pass an endotracheal tube. Case reports have highlighted an occurrence of severe neurological deficits, including permanent tetraplegia secondary to direct laryngoscopy in this patient population (8). AS involvement of the temporomandibular joint results in a narrowing of the joint space due to the presence of osteophytes and erosion of joint (9), which can severely impede mouth opening and impede any type of transoral approach to the larynx. Historically, it is believed that Pharaoh Ramses II (1303-1213 BCE) had AS. His neck had to be hyperextended to fit into his sarcophagus (Figure 2), which resulted in cervical spinal fracture (Figure 3) (10).
Airway Management Considerations for Patients with Ankylosing Spondylitis
Airway management in the hospital setting for patients with AS requires an individualized approach, always consider the patient’s overall clinical condition, their specific airway anatomy, available equipment, and caregiver skills.
Patients with chronic cervical kyphosis from AS have a significant risk of neurological injury from any neck-extending procedure. Neck extension can also cause vertebrobasilar insufficiency resulting from bony encroachment on the vertebral artery. Injuries to the cervical spine and spinal cord after an emergency intubation in patients with AS, such as dislocation of C6 vertebra and tetraparesis, have been reported (12).
Direct laryngoscopy is associated with a low first pass success rate and a high complication rate in patients with AS; hence, this technique should be avoided whenever possible. However, video-laryngoscopes provide an easy learning curve with reasonable effectiveness and safety comparable to standard fiberoptic intubation in some situations (11). If the patient has a significant level of temporomandibular joint damage with limited oral opening, or significant fixed cervical spine deformities are present, the video-laryngoscope may not be any safer or effective than direct laryngoscopy. In these situations, fiberoptic intubation will be the best approach. In emergent situations, intubating LMA (I-LMA) will be helpful (14,15,20). The advantages of this technique are that laryngeal visualization is not necessary, the trachea can be intubated without head or neck movement, and ventilation of the patient’s lungs can be maintained during the procedure.
Other Considerations Regarding Care of Patients with Ankylosing Spondylitis
Pulmonary Considerations: Patients with AS may have restrictive lung disease due to fusion of costovertebral joints, which can limit chest expansion. Additionally, patients with AS may have pulmonary fibrosis, which often manifests the worst in the upper lobes. Therefore, pulmonary function tests and arterial blood gas analysis for patients with AS are advisable, especially during preoperative preparations.
Cardiac Considerations: In patients with AS, inflammatory involvement of the heart just under aortic valve can lead to aortic valvular insufficiency, or even complete heart block; thus, a preoperative electrocardiogram is mandatory, and an echocardiogram should be obtained to assess the severity of possible AS–associated valvular disease.
Complications Associated with Spinal Cord Injury in Patients with Ankylosing Spondylitis
In an analysis of 12,484 hospital admissions and 267 deaths in patients with AS, data abstracted from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample between 2007 and 2011 showed that c-spine fracture with spinal cord injury and sepsis led to the highest odds of death (16). Another recent analysis of the U.S. Nationwide Inpatient Sample data of years 2016-2018 of 5385 AS patients with spinal fractures found spinal cord injury was present in 26.5% of the patients with cervical spine fractures. The overall complication rate was 40.8%, highest in those with spinal cord injury. Respiratory complications, including pneumonia and respiratory insufficiency, were the predominant complications in the overall cohort.
Prone Positioning in Patients with Ankylosing Spondylitis
Without proper planning, these patients may experience disastrous outcomes, such as complete spinal cord damage and possible death. Prone positioning can lead to physiological damage to patients with AS if underlying restrictive lung disease or cervical spine fracture are present (16,17). Therefore, proper planning and discussion needs to take place between care teams if prone positioning is absolutely necessary. Ideally, special positioning beds with proper padding and head support should be used to maintain the curvature of spine, and any forcible movements of the neck in the presence of neuromuscular blockade should be avoided (18).
References
- Reveille JD, Witter JP, Weisman MH. Prevalence of axial spondylarthritis in the United States: estimates from a cross-sectional survey. Arthritis Care Res (Hoboken). 2012 Jun;64(6):905-10.
- Reveille JD, Weisman MH. The epidemiology of back pain, axial spondyloarthritis and HLA-B27 in the United States.Am J Med Sci. 2013 Jun;345(6):431-6
- Maurer K. Basic data on arthritis: knee, hip, and sacroiliac joints in adults ages 25–74 years, United States, 1971–1975. Vital Health Stat. 1979;11(213):1–31.
- Truumees, et al. 2018. Orthopaedic Knowledge Update: Spine 5. Lippincott Williams & Wilkins.
- El Maghraoui et al. “Cervical Spine Involvement in Ankylosing Spondylitis.” Clinical Rheumatology 2003; 22 (2): 94–98.
- Prevalence and risk factors of osteoporosis and vertebral fractures in patients with ankylosing spondylitis. Bone 2009; 44:772-6.
- Ognjenovic M, Raymond WD, Inderjeeth CA, Keen HI, Preen DB, Nossent JC. The Risk and Consequences of Vertebral Fracture in Patients with Ankylosing Spondylitis: A Population-based Data Linkage Study.J Rheumatol. 2020 Nov 1;47(11):1629-1636.
- Oppenlander, et al. “Catastrophic Neurological Complications of Emergent Endotracheal Intubation: Report of 2 Cases.” Journal of Neurosurgery Spine; 2015 22 (5): 454–58.
- Arora et al. “Temporomandibular Joint Involvement in Ankylosing Spondylitis.” BMJ Case Reports 2013 (May). https://doi.org/10.1136/bcr-2013-009386.
- Feldtkeller et al. Ankylosingspondylitis in the pharaohs of ancient Egypt Rheumatol Int. 2003 Jan;23(1):1-5.
- Lai et al. The use of the Glidescope® for tracheal intubation in patients with Ankylosing Spondylitis. British Journal of Anaesthesia 2006; 97: 419– 22.
- Lu et al. The intubating laryngeal mask airway in severe ankylosing spondylitis. Canadian Journal of Anaesthesia. 2001; 48: 1015– 9.
- Asai et al. Placement of the intubating laryngeal mask is easier than the laryngeal mask during manual in‐line neck immobilisation. British Journal of Anaesthesia 1999; 82: 712– 4.
- Ciurea A et al. Impact of the COVID-19 pandemic on the disease course of patients with inflammatory rheumatic diseases: results from the Swiss Clinical Quality Management cohort. Annals of the Rheumatic Diseases. Volume: 80, Issue: 2, pp 238-241.
- Sanchez-Piedra et al. Clinical features and outcomes of COVID-19 in patients with rheumatic diseases treated with biological and synthetic targeted therapies. Ann Rheum Dis. 2020 Jul;79(7):988-990.
- Caron T, Bransford R, Nguyen Q, Agel J, Chapman J, Bellabarba C. Spine fractures in patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64.
- Wysham KD, Murray SG, Hills N, Yelin E, Gensler LS. Cervical Spinal Fracture and Other Diagnoses Associated With Mortality in Hospitalized Ankylosing Spondylitis Patients. Arthritis Care Res (Hoboken). 2017 Feb;69(2):271-277.
- AlMutiri AM, Alsulaimani S, Sabbagh AJ, Bajunaid KM, Tashkandi WA, Baeesa SS. Cervical Spinal Cord Injury During Prone Position Ventilation in the COVID-19 Pandemic. Cureus. 2021 Oct 21;13(10):e18958. doi: 10.7759/cureus.18958
- Caron et al. Spinefracturesin patients with ankylosing spinal disorders. Spine (Phila Pa 1976). 2010 May 15;35(11):E458-64
- Lucas DN, Yentis SM. A comparison of the intubating laryngeal mask tracheal tube with a standard tracheal tube for fibre‐optic intubation. Anaesthesia 2000; 55: 358– 61.
- Tan, et al. “Syndesmophyte Growth in Ankylosing Spondylitis.” Current Opinion in Rheumatology 2015; 27 (4): 326–32.

Figure 1. Lateral Cervical Spine Radiograph of a Patient with Advanced AS. Note the Fusion of the Apophyseal Joints Posteriorly and of the Outer Fibers of the Annulus Fibrosus Anteriorly

Figure 2. The Remains of Pharaoh Ramses II, Indicating the Pre-Mortem Position of the Neck and the Forced Hyperextension of the Cervical Spine to Fit into the Sarcophagus
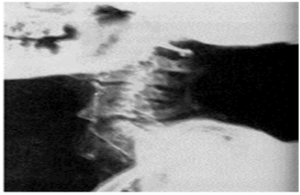
Figure 3. Lateral Spinal Radiograph of Ramses II: The Results of Forced Hyperextension of a Fused Cervical Spine
Authors



Categories
- Announcements
- Annual Meeting
- Award
- Book & Media Reviews
- Call for Articles
- Case Reports
- Clinical Research Consortium
- Committee Reports
- Council Report
- COVID-19
- DEI
- Early Career Intensivists
- Editor’s Message
- Featured Articles
- Fellows
- Jobs
- Literature Survey
- Match Applicants
- Medical Ethics
- Member Essays
- Member Spotlight
- Opinion
- Patient Safety Series
- PDAC
- President’s Corner
- Private Practice
- Pro/Con
- Research Updates
- Social Media Highlights
- Submission Guidelines
- Topical Review
- Wellness Series
- White Papers
- Women in Critical Care
- Work-Life Balance
Current Newsletter

Past Newsletters
Drip
















ASA 2023 Annual Meeting







September is Women in Medicine Month and throughout the month, four of our members will be sharing their experiences as a woman in critical care.




IARS & SOCCA Abstracts 2023
Abstracts of International Anesthesia Research Society & Society of Critical Care Anesthesiologists 2023 Annual Meetings are available in the May 2023 issue of Anesthesia & Analgesia.

Podcasts
SOCCA Women in Critical Care has collaborated with Stanford Continuing Medical Education for a Stanford Medcast Women in Critical Care podcast mini-series.
Episode #66—”Psychosocial Challenges Facing Physicians”—stream now
SOCCA polled the WICC and got the answers we wanted to hear about. We hope this episode helps at least one person out there!
If you have 21 minutes, listen and get your CME credit!

Episode #65—”Stereotype Threats”—stream now

Episode #63: “The Wicked Problem of Physician Well-Being”—stream now

Episode #59—“Underestimation of Influence”—stream now



